

What is Population Health Management anyway?

In thinking about my last entry on recommendations, I've gotten to thinking a little more deeply about the broader term Population Health. Population Health is a term that has been used increasingly since the passage of the Affordable Care Act. But what does it mean?
In a 2013 report from Academy Health-- the lobbying arm of Health Services researchers, they share an interesting conundrum:
The phrase “population health” is increasingly used by researchers, practitioners, and policymakers in health care, public health, and other fields. Although their understanding of this phrase differs, many see attention to population health as a potent opportunity for health care delivery systems, public health agencies, community-based organizations, and many other entities to work together to improve health outcomes in the communities they serve.
So we don't agree on exactly what it means, but it represents a great opportunity! As insane as this sounds, I know exactly what they mean.
Regardless of whether you are a payor, provider, public health worker, government official, or simply a thoughtful person, it has probably occurred to you that we can take better care of our population beyond the one at a time model prevalent in medical care. Hence the idea of focusing on population health.
Past that, the term breaks down a little bit, and there may be a way to put it back together.
First of all, who is in your population? It depends on who you are-- a payor has members, governments have constituents, public health workers have jurisdictions, primary care providers have panels (sort of). Let's assume you can figure this out and manage all of the challenges of constantly updating a list. An aside--it is amazing how difficult keeping an updated accurate list of names still is in the technologically marvelous era in which we currently live. Just look at your last formal party invite list and weep at how many people have moved, married, lost your friendship, etc. So you have your population, how do you manage their health?
Let's start with an example from the medical system. What we have done in health care for the longest time is reactive, serial care, synchronous care. That is to say, we generally take care of people, one at a time, as they make appointments with us. The performance of our health care system suggests that this is not a great way to improve the health of individuals or populations.
One common suggestion in the primary care world is the "registry." Simply put-- what if we had a list of everyone in our population with a given condition, like diabetes (it is ALWAYS diabetes). We could work on those patients getting their foot exams, eye exams, A1c, and other things done for their diabetes without waiting for them to come in to us. We can shift from being reactive to being proactive. Problem solved, population managed.
Or have we simply changed from one list of patients that we care for one at a time (appointment list) to a different, and possibly better list (diabetes registry).
On the other end of the spectrum is the public health opinion-- big changes that affect everyone at once. For instance, great roads. I studied medicine and public health in New Orleans and had the great fortune to learn from Larry Durante. It turns out in nearby Metairie, we had the 9th most dangerous intersection in America in 2001. The medical system likely worked overtime to absorb all of the car accident victims with better ambulances, trauma bays, surgeries, rehabs, etc. But it was "fixing the damn intersection" as Dr. Durante put it, that actually solved the problem. Here we did one thing and helped lots of people by preventing a problem.
So now we have a few ends of the spectrum here, all of which fall somewhere into population management. In fact, there is a group out of Duke trying to marry the shockingly different disciplines of health care and public health.
But what if we dive a little deeper into the definition?
Perhaps to resolve some of the confusion, we separate Populate Health Management into its constituent parts:
Population Health Measurement or How is our population doing?
Population Health Interventions or What are we doing to make them better?
Separating into these categories may begin to resolve the tension between the measurers (traditionally government and payors) and the doers (health care and public health).
The measurement piece is crucial, because if you cannot measure you cannot improve. Getting measurements correct, getting accurate data and in a way that does not impede the actual care of a population is crucial. Being more in the doer camp, I'd like to come back to measurement in the future.
When it comes to the doing then, we have a few choices on how to frame our work. How do we reconcile population health as both a better list of patients and fixing an intersection? For that, why not a two-by-two table? (I have no art department as of yet, and I use the word patient because, well, I am a doctor).
Population Health Intervention Types:
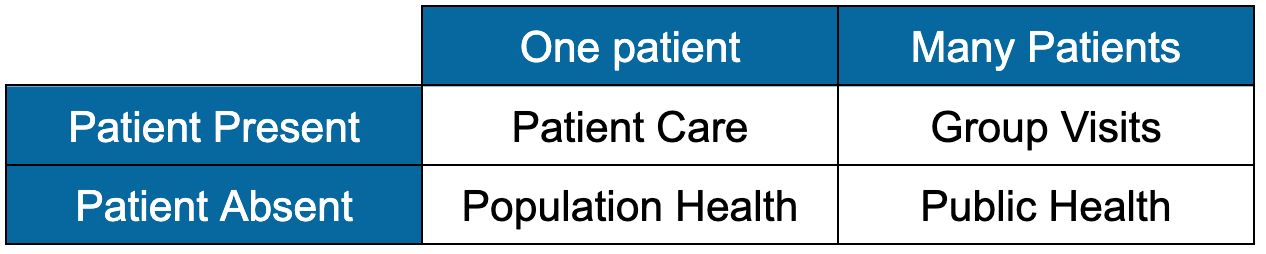
In this framework, we can think of doing things that affect one patient at a time, like a doctor's visit vs. things that affect many patients at a time, like fixing an intersection. However, whether or not the individual(s) are present makes a big deal in terms of the type of intervention. For example, a doctor's visit is helps a single, present patient. It goes in the top left. The intersection fixing helps many patients, all of whom were doing something better with their time when the intersection was fixed--that falls into the bottom right.
What can we extrapolate from this? Let's go back to our list of diabetics. We can decide to see them all in clinic soon, top left. We can decide to form a diabetes group and have a bunch in our office at once, top right. We can text each patient who is overdue for an eye exam, bottom left. Or we can tweet an informational piece to all of our diabetics, bottom right.
In this way we can begin to categorize interventions based on their effect size and presence requirements, and start solving problems with solutions from the proper quadrant. Going back to Metairie, the health system built up capacity to better serve one patient at a time, at potentially huge expense and in no way decreasing the ill effects of the intersection. We had a lower right problem with an upper left solution.
Where else in our work can we just "fix the damn intersection?"